From the beginning of this crisis we have been pointing out that there are two mutually contradictory messages at the heart of the covid19 rollout, and, just as Orwell describes in 1984, a major point of the exercise seems to be to get people to believe both at the same time.
1. ‘BE AFRAID…’
The first message is that covid19 is terrifying, unique, an existential threat to the human race.
This message is never sourced to much fact, because the facts about the virus don’t really support it. If it cites anything solid it’s the appallingly sloppy and discredited Imperial computer model, or some generic research into the pathology of severe infections or rare viral syndromes, which it tries to spin as being unique to covid19, even though it is not. But mostly it doesn’t cite anything at all. Or really claim anything at all.
It just tells people to be afraid. Very afraid. Of death, of uncertainty, of the ‘virus’, of other people, of ‘fake news’.
The fear being encouraged is not rooted in facts, and is therefore impervious to them.
2. ‘THERE IS NOTHING TO BE AFRAID OF…’
The second message is that covid19 is actually pretty harmless and no big deal.
This message is rooted in a great deal of fact, because, as we have been pointing out since day one, pretty much all the data coming out about this virus supports exactly this conclusion.
No official body has ever denied this, and most of them readily admit it. Regularly and unambiguously. Here and here and here and here.
Chris Whitty above is only one of many and this is not even his first go (see here) at explaining clearly that covid19 is only dangerous to a very very small minority of people, and that most who get it will be just fine.
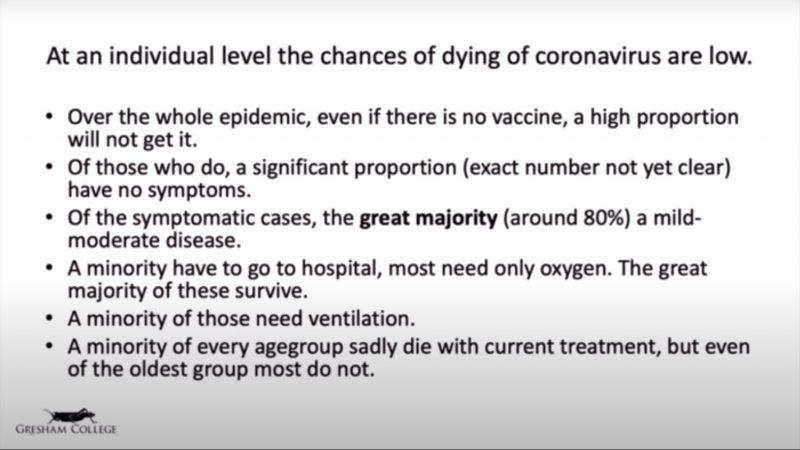
Here’s a slide from his talk on April 30th:
Now, let’s look at what he is saying in the above video, on May 11th [our emphasis]:
[T]he great majority of people will not die from this and I’ll just repeat something I said right at the beginning because I think it’s worth reinforcing:
Most people, a significant proportion of people, will not get this virus at all, at any point of the epidemic which is going to go on for a long period of time.
Of those who do, some of them will get the virus without even knowing it, they will have the virus with no symptoms at all, asymptomatic carriage, and we know that happens.
Of those who get symptoms, the great majority, probably 80%, will have a mild or moderate disease. Might be bad enough for them to have to go to bed for a few days, not bad enough for them to have to go to the doctor.
An unfortunate minority will have to go as far as hospital, but the majority of those will just need oxygen and will then leave hospital.
And then a minority of those will end up having to go to severe end critical care and some of those sadly will die.
But that’s a minority, it’s 1% or possibly even less than 1% overall.
And even in the highest risk group this is significantly less than 20%, ie. the great majority of people, even the very highest groups, if they catch this virus, will not die.
And I really wanted to make that point really clearly…
It seems all the officials want ‘to make that point really clearly’, even while they behave as if it was not true.
Why?
There’s plenty of room for speculation there, and we leave it to readers to get into that BTL.
The motives, though, are less important than the basic and undeniable fact – the fear currently gripping the public mind is being simultaneously encouraged and acknowledged as unnecessary by the bodies overseeing the ‘response’.
And if enough people would wake up to the pea-and-thimble trick being pulled on them, then the most dangerous and far-reaching coup against human liberty we have ever seen would essentially be stopped in its tracks.
More soldiers died from disease than bullets during WWI.
The Spanish Flu was neither Spanish nor Flu. According to a 2008 study by the U.S. National Institute of Health, the “predominant” killer in 1918-19 was bacterial pneumonia, and the first cases were not in Spain.
Initial outbreaks can be traced to U.S. military bases. A bacterial vaccine experiment on soldiers at Fort Riley, Kansas is one of the military epicenters of the epidemic.
The serums, anti-toxins and vaccines used on soldiers were made in horses at the Rockefeller Institute in New York (and in NJ). The same horses were used “in the preparation of diphtheria, tetanus antitoxin and antimeningococcus serum.” Same horses, multiple pathogens.
When WW1 ended on November 11, 1918, soldiers returned to their home countries and colonial outposts, spreading the killer bacterial pneumonia worldwide.
During WW1, the Rockefeller Institute also sent similar batches of the antimeningococcus serum used at Fort Riley to England, France, Belgium, Italy and other countries.
Vaccine experiments like the WWI experiments on soldiers in WW1 are not a thing of the past. Watch as Dr. Stanley Plotkin,(2) the Godfather of the US vaccine program, describes his vaccine experiments on the mentally handicapped, orphans, children of mothers in prison. Dr. Plotkin expresses a preference for experimenting “on children and adults who are human in form but not in social potential.” The deposition was taken in January 2018.
In Part 1, I asked if medical products made in horses may have played a role in the new disease which killed millions worldwide in the pandemic of 1918-19.
The feature article, “How New York City’s Health Department Makes Serums and Vaccines for the United States Army” describes processes in place in 1917:
“After the horse has been inoculated with the disease poison in gradually increasing doses he is bled and his serum is found to be antitoxin.
This is administered to human beings and renders them immune to the disease …. Some horses give more antitoxin serum than others.
The same horse may be used at several different times for the preparation of distinctly different antitoxins … Horses are used in the preparation of diphtheria, tetanus antitoxin and antimeningococcus serum. “
It is difficult to believe that they used the same horses to make multiple disease serums, but they did.
If safety had been a concern, perhaps certain horses would have been dedicated to producing serum for one disease (or “poison” as the article calls it), but safety does not appear to be on the list of concerns.
These muddled and potentially contaminated serums were then given to soldiers (and to the public).
SPECIES JUMP?
Were pathogens transferred from these horses to humans in mass quantities in ways they had never transferred before?
Humans and horses had interacted closely for centuries, but horse serum had not been injected into humans in that way before, bypassing the human immune system.
Is it possible that this new method of exposure caused the bacterial pneumonias which ripped human lungs apart in ways never seen before?
Could pathogens relatively harmless to horse lungs make a species-jump and destroy human lungs?
“In 1919, Bemelmans’s argument on the identical nature of human and horse influenza in the Nederlandsch Tijdschrift voor Geneeskunde (the Dutch medical journal) was reviewed in the veterinary journal,
… in 1914 he extended his theory on horse flu to several human and animal infectious diseases in an article in the Dutch medical journal. Bemelmans listed human influenza as an example among many other animal and human diseases which he thought were accompanied by (deadly) infections of streptococci.
Although he did not yet argue that human and horse flu were exactly equal, he did explicitly note their similarities: ‘Also between the human influenza and the so-called breast disease in horses peculiar similarities exist’…
Dr. Bemelmans’s contemporaneous observations have largely been lost to history, in part because of the self important attitude of the medical community.
The hubris of the medical community prevented them from listening to a lowly veterinarian.
However, Dr. Bemelmans’s observations and persistence in getting them published are extraordinarily valuable. His awareness at the time that bateria was the killer of both humans and horses in the pandemic of 1918-19 put him decades ahead of his contemporaries.
If Dr. Bemelmans was correct that horses and humans were suffering from an identical disease, are there diseases identical (or very similar) in both horses and humans? Do any of those diseases target the lungs?
In a 1969 paper, Kansas State University veterinarian Dr. Charles E. Cornelius compiled a list of diseases which were very similar or identical in humans and various other species. Among the diseases identical/very similar in humans and horses is pulmonary emphysema, which targets the lungs.
Did a pathogen which causes pulmonary emphysema “species-jump” from horses to humans in these serums and vaccines?
The vaccines were obviously manufactured in primitive, unavoidably unsafe conditions and then given to WW1 soldiers as an experiment.
What exactly was in the serums and vaccines made in the horses at the Rockefeller Institute – especially considering that the same individual horses were used to for variety of serums for multiple diseases?
Recall from Part 1 that Streptococci bacteria were commonly found in the tissue samples from the autopsies of those who died in 1918-19. (5)
Cornelius said human and horse pulmonary emphysema are identical. Bemelmans reported that humans and horses were suffering from the same disease.
Did doctors treating soldiers suffering from “Spanish Flu” report on encountering a new killer type of pulmonary emphysema, causing lung damage that they had ever seen before?
Captain Dr. Torrey served at Camp Hancock, just outside of Augusta, GA. The soldiers who came through Camp Hancock were likely on their way to Charleston, SC to board ships to France, but many of them would not survive to get to the front.
Thousands died at Camp Hancock. Some who survived the illness likely made it to the ships, potentially passing the infectious bacteria to other soldiers in the unsanitary conditions which were rampant during WWI.
From Dr. Torrey’s report:
“Summary
… Certain conditions were invariably present, including an intense bronchitis and peribronchitis similar to that found in a previous epidemic of pure hemolytic streptococcus infection (Scarlet Fever). There was also present from the first a destructive softening of the lung parenchyma.
In addition to this there was always an early and persisting generalized pulmonary emphysema which frequently was the main factor in causing death by interference with the mass movement of venous blood.
These conditions were found in every case examined at autopsy. Except for frequent otitis media (ear infection) there were almost no complications or sequelae outside of the chest.
The pulmonary emphysema, with consequent venous stasis, accounted for the cyanosis (turning blue/purple color), epistaxis (nosebleeds) and fixation of the chest in the phase of extreme inspiration (inhaling), with low stand of the diaphragm, which characterized these cases, and also accounted for the paradoxical physical signs (paradoxical breathing) in which fluid developed in the chest.”
Torrey describes what happened to these soldiers as they died. They were coughing, becoming “cloud adults” (8) (as described in Part 1).
It looked like a bacterial infection to him. Autopsies showed lung tissue had been damaged, which restricted blood flow, turning the dying a bluish/purple color, due to lack of oxygen.
FLUID IN THE LUNGS STRANGLED THE HUMAN VICTIMS OF SPANISH FLU – STRANGLES?
There is a highly contagious horse respiratory infection called Strangles (or Distemper). If this disease can kill horses, what would it do to human lungs if introduced into humans, via injection and therefore bypassing the immune system, on a mass scale?
Did streptococcus equi contaminate the serums and vaccines made in horses produced at the Rockefeller Institute and injected into soldiers in a vaccine experiment? Was streptococcus equi in the medical serums given to the soldiers as treatments? Was it some other pathogen which species jumped?
Did medical hubris lead to a mistake which caused a species jump which killed 50-100 million people 100 years ago?
WHAT NOW?
The vaccine industry is always looking for human test subjects. They have the most success when they are able to find populations who are not in a position to refuse. Soldiers (11), infants, the disabled, prisoners, those in developing nations – anyone not in a position to refuse.
Vaccine experimentation on vulnerable populations is not an issue of the past.
Watch this video clip of Dr. Stanley Plotkin where he describes using experimental vaccines on orphans, the mentally retarded, prisoners, and those under colonial rule.
The deposition was in January 2018.
The hubris of the medical community is the same or worse now than it was 100 years ago.
Watch as Dr. Plotkin admits to writing,
“The question is whether we are to have experiments performed on fully functioning adults and on children who are potentially contributors to society or to perform initial studies in children and adults who are human in form but not in social potential.”
In part because the global community is well aware of medical hubris and well aware of the poor record of medical ethics, the Universal Declaration on Bioethics and Human Rights (13) developed international standards regarding the right to informed consent to preventative medical procedures like vaccination.
The international community is well aware that the pharmaceutical industry makes mistakes and is always on the lookout for human test subjects.
The Declaration states that individuals have the human right to consent to any preventative medical intervention like vaccination.
Article 3 – Human dignity and human rights
1. Human dignity, human rights and fundamental freedoms are to be fully respected.
2. The interests and welfare of the individual should have priority over the sole interest of science or society.
Article 6 – Consent
1. Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned, based on adequate information. The consent should, where appropriate, be express and may be withdrawn by the person concerned at any time and for any reason without disadvantage or prejudice. (13)
Clean water, sanitation, flushing toilets, refrigerated foods and healthy diets have done and still do far more to protect humanity from infectious diseases than any vaccine program. Doctors and the vaccine industry have usurped credit which rightfully belongs to plumbers, electricians, sandhogs, engineers and city planners.
For these reasons, policy makers at all levels of government should protect the human rights and individual liberties of individuals to opt out of vaccine programs via exemptions.
The hubris of the medical community will never go away. Policy makers need to know that vaccines like all medical interventions are not infallible. Vaccines are not magic. We all have different susceptibility to disease. Human beings are not one size fits all.
In 1918-19, the vaccine industry experimented on soldiers, likely with disastrous results.
In 2018, the vaccine industry experiments on infants every day. The vaccine schedule has never been tested as it is given. The results of the experiment are in: 1 in 7 American children is in some form of special education and over 50% have some form of chronic illness. (14)
In 1918-19, there was no safety follow up after vaccines were delivered.
In 2018, there is virtually no safety follow up after a vaccine is delivered. Who exactly gave you that flu shot at Rite Aid? Do you have the cell number of the store employee if something goes wrong?
In 1918-19, there was no liability to the manufacturer for injuries or death caused by vaccines.
In 2018, there is no liability for vaccine manufacturers for injuries or death caused by vaccines, which was formalized in 1986. (15)
In 1918-19, there was no independent investigative follow up challenging the official story that “Spanish Flu” was some mystery illness which dropped from the sky.
I suspect that many of those at the Rockefeller Institute knew what happened, and that many of the doctors who administered the vaccines to the troops knew what happened, but those people are long dead.
In 2018, the Pharmaceutical industry is the largest campaign donor to politicians and the largest advertiser in all forms of media, so not much has changed over 100 years. This story will likely be ignored by mainstream media because their salaries are paid by pharmaceutical advertising.
The next time you hear someone say “vaccines save lives” please remember that the true story of the cost/benefit of vaccines is much more complicated than their three word slogan.
Also remember that vaccines may have killed 50-100 million people in 1918-19. If true, those costs greatly outweighed any benefit, especially considering that plumbers, electricians, sandhogs and engineers did, and continue to do, the real work which reduces mortality from disease.
Vaccines are not magic.(16) Human rights and bioethics are critically important. Policy makers should understand the history of medical hubris and protect individual and parental human rights as described in the Universal Declaration on Bioethics and Human Rights.
——————–
Kevin Barry is the President of First Freedoms, Inc. a 501.c.3. He is a former federal attorney, a rep at the UN HQ in New York and the author of Vaccine Whistleblower: Exposing Autism Research Fraud at the CDC. Please support his work at http://www.firstfreedoms.org
4. Haalboom, F., 2014. ‘Spanish’ flu and army horses: what historians and biologists can learn from a history of animals with flu during the 1918–1919 influenza pandemic. Studium, 7(3), pp.124–139. DOI: http://doi.org/10.18352/studium.9830
9. Deaths from Bacterial Pneumonia during 1918–19 Influenza Pandemic
John F. Brundage* and G. Dennis Shanks†
Author affiliations: *Armed Forces Health Surveillance Center, Silver Spring, Maryland, USA; †Australian Army Malaria Institute, Enoggera, Queensland, Australia https://wwwnc.cdc.gov/eid/article/14/8/07-1313_article
Leaving a lucrative career as a nephrologist (kidney doctor), Dr. Suzanne Humphries is now free to actually help cure people.
In this autobiography she explains why good doctors are constrained within the current corrupt medical system from practicing real, ethical medicine.
One of the sane voices when it comes to examining the science behind modern-day vaccines, no pro-vaccine extremist doctors have ever dared to debate her in public.
Despite early exposure, its dense and aging population, and little social distancing measures, Japan reports low infection and low death from COVID‐19. Here, we speculate on and discuss the possible reasons that may account for this anomaly.There is a lot of interest brewing as to why Japan has such low numbers of confirmed infected cases of the COVID‐19 disease, caused by the SARS‐CoV‐2 virus (Fig 1), despite its high population density (over 6,100 persons/sqkm in Tokyo, 2.4 times higher than New York City) and large percentage of high‐risk individuals over 65 years of age (about 26%, compared with 15% in the USA). In Singapore and Hong Kong, rapid and strict quarantine rules and contact tracing have helped to “flatten the curve”. In South Korea, mass testing and quarantine measures appear to have reduced the rate of new cases. However, Japan has not engaged in expansive testing, contact tracing, or strict quarantine measures and yet is reporting a slow growth rate of infected persons and a death rate that is currently just 1/10th of world average. It is difficult to make direct comparison of infection rates, because the number of tests per capita varies dramatically between countries. However, this low death rate cannot be simply explained by lack of testing or reporting, as no surge in death from respiratory syndromes has been reported either.
Figure 1.Cumulative number of cases, by number of days since February 1, 2020
So how has Japan dealt with COVID‐19? The Japanese Cluster Response Team of the Ministry of Health set forth on March 9th a three‐pronged approach.
early detection of and early response to infection clusters
early patient diagnosis and enhancement of intensive care and the securing of a medical service system for the severely ill
behavior modification of citizens (including advise to refrain from holding large‐scale events, temporary school closures)
Note that none of these involve strict social distancing measures taken by other countries. Why is this? What can we learn from Japan to help flatten the curve in other countries?
Here, we discuss several hypotheses and provide arguments for or against each hypothesis.
1.Japanese culture is inherently suited for social distancing, and face mask use prevents viral spread.
It is certainly true that the Japanese customs do not involve handshaking, hugging, or kissing when greeting. In addition, many Japanese wear cloth or paper face masks (not the N95 respirators required for exclusion of aerosol viral particles) in the winter to avoid transmission of respiratory infections. People use the mask to avoid spreading the infection and also in an attempt to prevent exposure to infection. However, we are unconvinced that this is the main or only reason why COVID‐19 is so well contained in Japan. There is no social distancing in rush hour trains and buses, or when walking in crowded streets to school or to work. The use of face mask is also practiced in other Asian countries that witnessed higher rates of infection. A hint to whether this is a valid hypothesis comes from looking at other pandemic viral respiratory diseases. The community R0 rate for the 2009 pandemic flu for Japan was 1.28 while USA was 1.7–2.0 (Boelle et al, 2011). Thus, R0 in Japan was somewhat lower than the global median R0 of 1.47. In addition, an observational study of elementary school children in Japan found that wearing masks had significant protective association (odds ratio of 0.859, 95% confidence interval 0.778–0.949) against seasonal influenza (Uchida et al, 2017). Therefore, the social practice culture of Japan and mask use may explain to some extent the lower number of observed COVID‐19 cases, but is unlikely the only explanation.
2.Japanese people were exposed to a milder version of SARS‐CoV‐2 that conferred herd immunity before the spread of a more virulent strain of CoV2.
While possible, there is no current evidence that milder strains of SARS‐CoV‐2 exist. Nor do we know what sort of antibody response would develop as a result of exposure to such a hypothetical variant. Phylogenetic analysis of SARS‐CoV‐2 of more than 3,500 SARS‐CoV‐2 genomes from around the world, including 29 from Japan, suggests that the outbreak in Japan was sparked by several independent virus introductions primarily from China (https://nextstrain.org/ncov?f_country=Japan, accessed 7.4.2020) (Hadfield et al, 2018). Furthermore, all of the SARS‐CoV‐2 genomes are highly similar; most contain no more than 10 mutations compared to the virus that started the original outbreak. Thus, it is highly unlikely that the virus has evolved a significantly different phenotype, and even less likely that it was introduced early into Japan.
Notably, early cases in Japan (January–February) were all linked to virus introduced from China. Now, in March, the outbreaks in Japan are linked to introductions from Europe, and there is a large gap in between those early introductions in January and the recent ones in March. While the data are still limited, this suggests that Japan was able to control the early outbreaks, keeping cases down, but is now experiencing a second wave introduced more recently from Europe.
3.Japanese people have reduced susceptibility due to ACE2 receptor expression.
SARS‐CoV‐2 utilizes ACE2 as a receptor to enter cells. It is theoretically possible that ACE2 expression in the respiratory tract is somehow lower in the Japanese population, though no direct evidence was identified during studies investigating coronavirus S‐protein binding‐resistant ACE2 mutants among different populations. If anything, East Asian populations were reported to have higher allele frequency in the ACE2 variants associated with higher ACE2 expression in tissues (Cao et al, 2020). However, the only way to find out whether the expression of ACE2 is indeed different is through surface protein staining of lung tissues, which has yet to be done.
4.Japanese people have distinct HLA that confers immune resistance to CoV2.
Genome‐wide association studies (GWAS) conducted on disease susceptibility show that HLA is usually the top locus associated with disease. This is true for infectious diseases, autoimmunity, or neurological disorders. HLA stands for human leukocyte antigen and is also known as MHC, or major histocompatibility complex. These genes encode for proteins that present antigenic peptides to T cells. HLA class I presents antigenic peptides to CD8 T cells, while HLA class II presents peptides to CD4 T cells. HLA genes are the most highly polymorphic genes in the human genome. The variety in HLA enables our immune system to survey for maximal number of antigen peptides that are present in pathogens, so as to elicit robust cellular immune responses. Previous studies have identified HLA‐B*4601 to be associated with higher risk of developing SARS disease (Lin et al, 2003), based on a small number of cases. However, whether there are any HLA alleles that confer resistance to COVID‐19 and whether the allele frequency is higher in the Japanese population are unknown.
5.BCG vaccine used in Japan confers protection against COVID‐19.
Japan, like many other countries including China, Korea, India, and the Russian Federation, have mandatory childhood BCG vaccines against tuberculosis. These countries have so far a relatively low per capita death rate from COVID‐19 compared to countries that have no mandatory BCG vaccines (USA, Spain, France, Italy, The Netherlands). What further distinguishes Japan is that the BCG vaccine strain used in Japan, Brazil, and Russia is one of the original strains, while further modified BCG strains are used for vaccination in European countries. This association between BCG vaccination and apparent low COVID‐19 incidence in Japan has spurred the idea that these two things may be linked (for more discussions on this topic, visit https://www.jsatonotes.com/2020/03/if-i-were-north-americaneuropeanaustral.html and https://news.yahoo.co.jp/byline/kimuramasato/20200405-00171556/).
How would BCG, an attenuated bacterial vaccine completely unrelated to COVID‐19, provide protection? Michai Netea and colleagues hypothesized that the vaccine may boost “trained immunity” (Netea et al, 2016)—in other words, certain immune stimuli may induce a prolonged state of resistance against pathogens in general, by elevating the expression levels of resistance factors. Studies have shown that receipt of BCG vaccine was associated with a reduction in all‐cause mortality within the first 1–60 months: The average relative risks were 0.70 (95% confidence interval 0.49–1.01) from five clinical trials (Higgins et al, 2016). Furthermore, Netea and colleagues showed that BCG vaccination reduced the levels of viremia caused by the yellow fever virus live attenuated vaccine (Arts et al, 2018), and post‐BCG increase of IL‐1β production strongly correlated with lower viremia after yellow fever virus administration. A placebo‐controlled randomized clinical trial of 1,000 healthcare workers in The Netherlands has started, and a similar trial is planned to begin at the Max Planck Institute (de Vrieze, 2020). The outcomes of these trials will help us to understand whether and how BCG confers resistance to other pathogens including SARS‐CoV‐2.
Conclusion
There are many other theories to explain the low number of COVID‐19 cases in Japan, yet we still do not have enough information to determine the cause of this striking discrepancy. Clearly, we do not understand what causes these differences. Many of these hypotheses can be tested as suggested above, such as examining ACE2 expression levels in the respiratory tract, GWAS data on COVID‐19 susceptibility, and whether BCG vaccines indeed confer long‐term innate immune resistance to SARS‐CoV‐2. The three‐pronged approach by the Cluster Response Team of the Japanese Ministry of Health has thus far contained the spread of COVID‐19 by quickly identifying clusters of infections, testing, and quarantine of the infected individuals. A word of caution is whether this approach will work in cases where super‐spreaders ignite a large‐scale transmission, or when there are multiple clusters that occur throughout the country at once. Perhaps one of the reasons for the low number of cases in Japan might relate to lack of super‐spreader events to date. Just within the last 24 h, Japan has declared the state of emergency, as Tokyo faces more than 1,000 confirmed cases, more than double the number a week ago. Perhaps stronger social distancing measures are required to keep the curve flattened in Japan.
Acknowledgements
We wish to thank Dr. Hiroshi Iwasaki for research and providing key resources from Japanese media and postings. We also thank Dr. Hironori Funabiki for his informative Twitter postings on this subject.
Conflict of interest
The authors declare that they have no conflict of interest.
References
Arts RJW, Moorlag S, Novakovic B, Li Y, Wang SY, Oosting M, Kumar V, Xavier RJ, Wijmenga C, Joosten LAB et al (2018) BCG Vaccination Protects against Experimental Viral Infection in Humans through the Induction of Cytokines Associated with Trained Immunity. Cell Host Microbe23: 89–100.e5CrossrefCASPubMedWeb of Science®Google Scholar
Boelle PY, Ansart S, Cori A, Valleron AJ (2011) Transmission parameters of the A/H1N1 (2009) influenza virus pandemic: a review. Influenza Other Respir Viruses5: 306–316Wiley Online LibraryPubMedWeb of Science®Google Scholar
Cao Y, Li L, Feng Z, Wan S, Huang P, Sun X, Wen F, Huang X, Ning G, Wang W (2020) Comparative genetic analysis of the novel coronavirus (2019‐nCoV/SARS‐CoV‐2) receptor ACE2 in different populations. Cell Discov6: 11CrossrefCASPubMedWeb of Science®Google Scholar
Hadfield J, Megill C, Bell SM, Huddleston J, Potter B, Callender C, Sagulenko P, Bedford T, Neher RA (2018) Nextstrain: real‐time tracking of pathogen evolution. Bioinformatics34: 4121–4123CrossrefCASPubMedWeb of Science®Google Scholar
Higgins JP, Soares‐Weiser K, Lopez‐Lopez JA, Kakourou A, Chaplin K, Christensen H, Martin NK, Sterne JA, Reingold AL (2016) Association of BCG, DTP, and measles containing vaccines with childhood mortality: systematic review. BMJ355: i5170CrossrefPubMedWeb of Science®Google Scholar
Lin M, Tseng HK, Trejaut JA, Lee HL, Loo JH, Chu CC, Chen PJ, Su YW, Lim KH, Tsai ZU et al (2003) Association of HLA class I with severe acute respiratory syndrome coronavirus infection. BMC Med Genet4: 9CrossrefPubMedGoogle Scholar
Netea MG, Joosten LA, Latz E, Mills KH, Natoli G, Stunnenberg HG, O’Neill LA, Xavier RJ (2016) Trained immunity: a program of innate immune memory in health and disease. Science352: aaf1098CrossrefCASPubMedWeb of Science®Google Scholar
Uchida M, Kaneko M, Hidaka Y, Yamamoto H, Honda T, Takeuchi S, Saito M, Kawa S (2017) Effectiveness of vaccination and wearing masks on seasonal influenza in Matsumoto City, Japan, in the 2014/2015 season: an observational study among all elementary schoolchildren. Prev Med Rep5: 86–91CrossrefPubMedGoogle Scholar
de Vrieze J (2020) Can a century‐old TB vaccine steel the immune system against the new coronavirus?Google Scholar
“Too bad if someone thinks this (Digital Certificates) creates a privacy problem.” Bill Gates
The following is based almost entirely on two editions of the Corbett Report which is still available on Bitchute below.
The Bill & Melinda Gates Foundation spends tens of millions of dollars per year on media partnerships, sponsoring coverage of its program areas across the board. Gates funds The Guardian‘s Global Development website. Gates funds NPR’s global health coverage. Gates funds the Our World in Data website that is tracking the latest statistics and research on the coronavirus pandemic. Gates funds BBC coverage of global health and development issues, both through its BBC Media Action organization and the BBC itself. Gates funds world health coverage on ABC News.
When the NewsHour with Jim Lehrer was given a $3.5 million Gates foundation grant to set up a special unit to report on global health issues, NewsHour communications chief Rob Flynn was asked about the potential conflict of interest that such a unit would have in reporting on issues that the Gates Foundation is itself involved in. “In some regards I guess you might say that there are not a heck of a lot of things you could touch in global health these days that would not have some kind of Gates tentacle,” Flynn responded.
It was Gates who sponsored the meeting that led to the creation of Gavi, the Global Alliance for Vaccines and Immunization, a public-private partnership bringing together state sponsors and big pharmaceutical companies, whose specific goals include the creation of “healthy markets for vaccines and other immunization products.” As a founding partner of the alliance, the Gates Foundation provided $750 million in seed funding and has gone on to make over $4.1 billion in commitments to the group.
Gates is held up as a hero for donating $35.8 billion worth of his Microsoft stock to the foundation, but during the course of his “Decade of Vaccines,” Gates’ net worth has actually doubled, from $54 billion to $103.1 billion.
Gates provided the seed money that created the Global Fund to Fight AIDS, Tuberculosis and Malaria, a public-private partnership that acts as a finance vehicle for governmental AIDS, TB, and malaria programs.
When a public-private partnership of governments, world health bodies and 13 leading pharmaceutical companies came together in 2012 “to accelerate progress toward eliminating or controlling 10 neglected tropical diseases,” there was the Gates Foundation with $363 million of support.
When the Global Financing Facility for Women, Children and Adolescents was launched in 2015 to leverage billions of dollars in public and private financing for global health and development programs, there was the Bill & Melinda Gates Foundation as a founding partner with a $275 million contribution.
When the Coalition for Epidemic Preparedness Innovations was launched at the World Economic Forum in Davos in 2017 to develop vaccines against emerging infectious diseases, there was the Gates Foundation with an initial injection of $100 million.
But even the World Health Organization itself is largely reliant on funds from the Bill & Melinda Gates Foundation. The WHO’s most recent donor report shows that the Bill & Melinda Gates Foundation is the organization’s second-largest donor behind the United States government.
Imperial College in London released a COVID-19 report and that’s where most of our US leaders are getting the information they’re basing their decision making on. The report runs us through a few different ways this could turn out depending on what our responses are. If we don’t do anything to control this virus, over 80% of people in the US would be infected over the course of the epidemic, with 2.2 million deaths from COVID-19. The source of this nonsense was the Gates Foundation.
The Institute for Health Metrics and Evaluation in Bill Gates’ home state of Washington, helped provide data that corroborated the White House’s initial estimates of the virus’ effects, estimates that have been repeatedly downgraded as the situation has progressed.
Unsurprisingly, the Gates Foundation has injected substantial sums of money into both groups. This year alone, the Gates Foundation has already given $79 million to Imperial College, and in 2017 the Foundation announced a $279 million investment into the IHME to expand its work collecting health data and creating models.
Beyond just their frequent collaborations and cooperation in the past, Anthiny Fauci has direct ties to Gates’ projects and funding. In 2010, he was appointed to the Leadership Council of the Gates-founded “Decade of Vaccines” project to implement a Global Vaccine Action Plan—a project to which Gates committed $10 billion of funding. And in October of last year, just as the current pandemic was beginning, the Gates Foundation announced a $100 million contribution to the National Institute of Health to help, among other programs, Fauci’s National Institute of Allergy and Infectious Diseases’ research into HIV.
Also in October of last year, the Bill & Melinda Gates Foundation partnered with the World Economic Forum and the Johns Hopkins Center for Health Security to stage Event 201, a tabletop exercise gauging the economic and societal impact of a globally-spreading coronavirus pandemic.
And the charity of billionaire Microsoft founder Bill Gates and his wife Melinda is under criticism following the disclosure it’s substantially increased its holdings in the agribusiness giant Monsanto to over $23 million. Critics say the investment in Monsanto contradicts the Bill and Melinda Gates Foundation’s stated commitment to helping farmers and sustainable development in Africa. (We learned that the retrovirus XMRV (Xenotropic Murine Leukemia-Related Virus) can be triggered in those who got it from vaccines by taking GMO, food, pesticides and Glyphosates which are what Monsanto does.) XMRV causes cancer and is linked both to Chronic Fatigue Syndrome and to autism.
In January of 2010, Bill and Melinda Gates used the World Economic Forum at Davos to announce a staggering $10 billion commitment to research and develop vaccines for the world’s poorest countries, kicking off what he called a “Decade of Vaccines.”
But contrary to the Gates’ own PR spin that this $10 billion pledge was an unalloyed good and would save eight million lives, the truth is that this attempt to reorient the global health economy was part of a much bigger agenda. An agenda that would ultimately lead to greater profits for Big Pharma companies, greater control for the Gates Foundation over the field of global health, and greater power for Bill Gates to shape the course of the future for billions of people around the planet.
Gates helped develop the Global Vaccine Action Plan administered by the Gates-funded World Health Organization.
Gates helped found Gavi, the Vaccine Alliance, aiming to develop “healthy markets” for vaccine manufacturers. Gates helped launch Gavi with a $1 billion donation in 2011, going on to contribute $4.1 billion over the course of the “Decade of Vaccines.”
And so after Ebola (which was created in US Bio-labs as a bioweapon), the global health community talked a lot about this, a new type of vaccine platform called DNA/RNA that should speed things along.
And so this Coalition for Epidemic Preparedness Initiative [sic], CEPI, is three countries—Japan, Norway, Germany—and two foundations—Wellcome Trust, [who] we work with on a lot of things, and our foundation, the Gates Foundation—coming together to fund . . . actually trying to use that platform and make some vaccines. And so that would help us in the future.
What should be surprising is that this strangely specific and continuously repeated message—that we will not go “back to normal” until we get a vaccine in 18 months—has no scientific basis whatsoever. Medical researchers have already conceded that a vaccine for SARS-CoV-2 may not even be possible, pointing to the inability of researchers to develop any kind of immunization against previous coronavirus outbreaks, like SARS or MERS.
But even if such a vaccine were possible, serious concerns remain about the safety of developing, testing and delivering such an “amazing vaccine” to “the entire world” in this remarkably short time frame. Even proponents of vaccine development openly worry that the rush to vaccinate billions of people with a largely untested, experimental coronavirus vaccine will itself present grave risks to the public.
One of these risks involves “disease enhancement.” It has been known for over a decade that vaccination for some viral infections—including coronaviruses—actually enhances susceptibility to viral infection or even causes infections in healthy vaccine recipients.
This is no mere theoretical risk. As researchers who were trying to develop a vaccine for the original SARS outbreak discovered, the vaccine actually made the lab animals subjected to it more susceptible to the disease.
ANTHONY FAUCI: We’re gonna start ramping up production with the companies involved, and you do that at risk. In other words, you don’t wait until you get an answer before you start manufacturing. You at risk proactively start making it, assuming it’s gonna work.
GATES: Yeah, so there’s an approach called RNA vaccine that people like Moderna, CureVac and others are using that in 2015 we’d identified that as very promising for pandemics and for other applications as well. And so, if everything goes perfectly with the RNA approach, we could actually beat the 18 months.
So we are not allowed to return to a normal life until we accept a vaccine that is untested and is RNA based meaning it rewrites he human genome so if we have children who survive they will not exactly be human. This is a risk Gates and Fauci are willing to assume you are willing to take if vaccination were voluntary which it won’t be.
It’s making your cell do the work of creating this viral protein that is going to be recognized by your immune system and trigger the development of these antibodies. Our bodies won’t make a full-fledged infectious virus. They’ll just make a little piece and then learn to recognize it and then get ready to destroy the virus if it then later comes and invades us. It’s a relatively new, unproven technology. And there’s still no example of an RNA vaccine that’s been deployed worldwide in the way that we need for the coronavirus.
Rushing at “Warp Speed” to develop a new vaccine using experimental technology and then mass-producing and delivering billions of doses to be injected into “basically the entire world” before adequate testing is even done amounts to one of the most dangerous experiments in the history of the world, one that could alter the lives of untold numbers of people.
In the US, the Department of Health and Human Services issued a declaration that retroactively provides “liability immunity for activities related to medical countermeasures against COVID-19,” including manufacturers, distributors and program planners of “any vaccine, used to treat, diagnose, cure, prevent, or mitigate COVID-19.” The declaration was issued on March 17th but retroactively covers any activity back to February 4th, 2020, the day before the Bill and Melinda Gates Foundation announced an emergency $100 million to fund treatment efforts and to develop new vaccines for COVID-19.
The plan to inject everyone on the planet with an experimental vaccine is no aberration in Bill Gates’ envisioned “Decade of Vaccines.” It is its culmination.
The “Decade of Vaccines” kicked off with a Gates-funded $3.6 million observational study of HPV vaccines in India that, according to a government investigation, violated the human rights of the study participants with “gross violations” of consent and failed to properly report adverse events experienced by the vaccine recipients. After the deaths of seven girls involved in the trial were reported, a parliamentary investigation concluded that the Gates-funded Program for Appropriate Technology in Health (PATH), which ran the study, had been engaged in a scheme to help ensure “healthy markets” for GlaxoSmithKline and Merck, the manufacturers of the Gardasil and Cervarix vaccines that had been so generously donated for use in the trial:
There’s the Gates-founded and funded Meningitis Vaccine Project, which led to the creation and testing of MenAfriVac, a $0.50-per-dose immunization against meningococcal meningitis. The tests led to reports of between 40 and 500 children suffering seizures and convulsions and eventually becoming paralyzed.
There’s the 2017 confirmation that the Gates-supported oral polio vaccine was actually responsible for the majority of new polio cases and the 2018 follow up showing that 80% of polio cases are now vaccine-derived.
There’s the 2018 paper in the International Journal of Environmental Research and Public Health concluding that over 490,000 people in India developed paralysis as a result of the oral polio vaccine between 2000 and 2017. As we shall see next time, money is not the end goal of Gates’ “philanthropic” activities. Money is just the tool that he is using to purchase what he really wants: control. Control not just of the health industry, but control of the human population itself.
The goal is clear. We remain in lockdown until a second or even third economy destroying wave of Covid-19 sweeps the world. Unemployment and business failures will abound until living conditions approach those of Germany in 1923 and America in 1933. 3 million Americans starved to death in the 1930s. The side effects of a lockdown are far worse than the coronavirus, especially if we knew the real number of people dying from Covid-19 versus those dying with it. There is a difference between dying in an auto accident with a tee-shirt and dying from a drunk driver hitting your car. One is incidental, the other is causal.
So we are forced to accept an unproven RNA vaccine that rewrites the human genome at considerable risk because Bill Gates wants us to be injected with digital Certificates. Sounds like the Mark of the Beast. We all submit to the New World Order. We are not allowed to work, to travel, to assemble or to do anything at all without the knowledge and approval of Bill Gates, Big Pharma and the NSA. What could go wrong?
The unelected billionaires might want to commit mass murder and kill 6 to 7 billion people. We would be powerless to object. We would or the survivors of the genocide would become docile little slaves to be ruled over by our Overlords.
David Rothkopf wrote Superclass in 2008 in which he said that the West is run by Thirty Families and their 6,000 Minions. Lockdowns will destroy small businesses so the only employers remaining will be the Thirty Families, their Minions and the governments they own. That would give the controllers of our Digital Certificates all the authority they need to run roughshod over us. Maybe they are already developing RNA tools to reprogram what were human beings into a more docile species. At that point, the multi-billionaires could do whatever they wanted to do to the rest of us.
What is their sick motivation? Because they are bored and have grown tired of the wars they engineered to kill off the lower classes. Rewriting the human genome is just something to do to screw with humans.
Related Articles:
I mentioned the Thirty Families and their 6,000 Minions. Read more about that here:
The Thirty Families Made Plans For A Future Without You.
This will introduce you to the Bilderberg Society which is one mechanism of control for the Thirty Families. The 2020 annual Bilderberg conference has been postponed.
The two videos from James Corbett of the Corbett Report which are the basis of this article are available here though any errors are my own responsibility. Corbett is the best!!
With US President Donald Trump preparing to square off with presumptive Democratic nominee Joe Biden in the 2020 race, Americans might as well be choosing between Orwell and Huxley, Pink Floyd co-founder Roger Waters told RT.
Though the current US president is a “failed landlord” who somehow managed to become “the most powerful man in the Western world,” Biden, his likely rival, does not present a better option, Waters said in an interview with Rafael Correa, the former president of Ecuador who now hosts a show on RT Spanish.
“There’s no choice to be made by the American people, this is why the idea that the United States is a democracy is such a sham,” Waters said, adding that the Democratic Party ruined any chance for a real alternative when it “crushed” the Bernie Sanders campaign, as the socialist senator would not serve the interests of “the people who actually run the country” – Wall Street and the “war machine.”
But the “most dangerous thing” in the current political moment, Waters argued, is “propaganda” which seeks to transform “the truth” into an “extreme point of view,” citing the vicious treatment of WikiLeaks co-founder and anti-secrecy crusader Julian Assange as an example.
There’s been a debate continuing about which dystopia our current world is more like, Aldous Huxley’s ‘Brave New World’ or George Orwell’s ‘1984.’ But the one thing that is common… is propaganda, it’s the Ministry of Truth
‘US healthcare system designed for the rich’
Beyond the political system, US healthcare has also left many Americans with few options, with crippling medical bills a leading cause of middle-class bankruptcies, even amid the Covid-19 outbreak.
“New York has been terrible, but you would expect it because there’s no health service in the United States of America,” Waters said. “Well, there is a health service, but it’s only for the very wealthy, and in consequence, they’re completely unprepared to face something like this.”
The US has long been the world’s top coronavirus hotspot, counting nearly 1.3 million cases of the illness and more than 77,000 fatalities. Though the country boasts more intensive care beds per capita than much of the world, the healthcare systems of the hardest-hit areas – such as New York and New Jersey – have strained under the pandemic. At some hospitals in New York City, federal agencies and even the military have stepped in to deploy refrigerated mobile morgue trucks just to cope with the surge of deaths from the virus.
Even as new medicines are developed to combat the pathogen, around one in seven Americans say they would be unable to afford treatment, according to a recent Gallup poll, leaving tens of millions of citizens largely helpless during a major health crisis.
On a more optimistic note, the rockstar said greater numbers of people are taking notice of corrupt political leaders and their media allies, not only in the United States but around the world, predicting that protests will again erupt in the streets once the pandemic crisis dies down, especially across Latin America.
“So there is a light. It’s a long, narrow tunnel, but there is more than a pinprick of light,” he continued. “The walls of the tunnel are crumbling because the people are demanding it.”
By Pablo Vivanco, a journalist and analyst specializing in politics and history in the Americas, who served as the Director of teleSUR English. Recent bylines include The Jacobin, Asia Times, The Progressive and Truthout. Follow him on Twitter @pvivancoguzman
28 Apr, 2020
Havana has punched above its weight for decades when it comes to health. But never have the differences between its socialist system and the market-based system of its strongest detractor, America, been so apparent.
Even before it reported novel coronavirus cases of its own in March, Cuba’s fingerprints were all over the efforts to stem the global pandemic, from China’s use of antivirals developed on the island to treat the infected, to the docking of a British cruise ship in Havana in order to allow the 1,000 people on board – including five Covid-19 carriers – to return home.
The MS Braemar, filled mostly with British citizens, was refused permission to disembark at several ports it approached. According to some reports, the US – a principal British ally – was one of the countries that turned it down. The ship’s operator, Fred. Olsen Cruise Lines, has not commented on the US specifically, saying they explored a number of options and would not disclose the details of those negotiations. The fact that the vessel ultimately found refuge on Cuba’s shores serves to illustrate the difference in approaches to this pandemic.
Despite considerable risk factors, including a high percentage of people over the age of 60 and a high number of visitors to the country, Cuba has been able to keep Covid-19 cases to just under 1,370 as of April 27, with just 54 deaths.
This is largely due to the fact that the Caribbean island not only has the highest ratio of doctors to population in the world, but also a free, universal health system based on proactive, community response.
The measures that began in January included training and preparation for medical professionals and facilities, but by March these extended into other sectors and included a virtual shutdown of the tourism industry – a huge chunk of Cuba’s economy.
Still, authorities maintained that Cuban doctors would continue to go to countries that needed support in controlling the spread of the virus. These same medical brigades were instrumental in supporting African nations in curbing and controlling the Ebola outbreak that began in 2014.
But now, for the first time, Cuban doctors have been received with open arms in European countries like Italy and Andorra, and they have even been welcomed back by some of the very same US-allied governments in Latin America that vilified and kicked them out just months ago.
The number of Cuban-trained doctors working in other countries is even higher when you count the graduates from Havana’s Latin American School of Medicine, which has provided free education to 35,000 doctors in 138 countries since 1999.
All of this has been accomplished under the severe limitations and resources that are the intentional consequence of barbaric US sanctions, which were recently intensified by the Trump administration.
Exporting its doctors and nurses abroad is a vital revenue-earner for Cuba. It brings in around $11 billion each year – a bigger source of income than the island’s tourism industry. At any one time, there are around 50,000 Cuban doctors working across 67 countries, an ‘army of white coats’, as officials describe them.
But while Cubans have put themselves in harm’s way to support people and countries all over the planet, the US has been doing the exact opposite.
In an audacious demonstration of hypocrisy, Washington has pressured countries to not accept Cuban doctors, while offering little support of its own, and has also deliberately (and perhaps illegally) seized shipments of medical equipment meant for other countries, including some of its closest allies.
#Cuba offers its international medical missions to those afflicted with #COVIDー19 only to make up the money it lost when countries stopped participating in the abusive program. Host countries seeking Cuba’s help for #COVIDー19 should scrutinize agreements and end labor abuses.
— Bureau of Democracy, Human Rights, and Labor (@StateDRL) March 24, 2020
To be fair, even if it had the will, the US government is not in a position to lend much support to anyone at the moment.
The weaknesses of America’s health system, which paradoxically has the highest per capita funding in the world by far, were laid bare even before the pandemic, as Democratic presidential hopefuls outlined their plans to provide adequate healthcare to the more than 70 million Americans who lack it.
Just a few weeks into this crisis, the picture is even bleaker, with millions more losing access due to job losses, and hospitals lacking proper equipment for patients and staff.
After weeks of New York splitting and sharing ventilators, Trump proclaims: “We are now the king of ventilators… We have handled the situation tremendously well.”This NYT story is from March 26: ‘The Other Option Is Death’ https://t.co/E4ZPkfxS2d
Holy freaking hell. A nursing manager at Mt Sinai Hospital in NYC just died from coronavirus. Nurses at the hospital have been wearing trash bags because of the lack of protective gear. https://t.co/DSkHKVECmEpic.twitter.com/gl3w7ksPog
To make matters worse, the discrepancy in measures at the state and local level demonstrates that the country’s overall response is nothing less than schizophrenic. Meanwhile, decisions from the White House – including having tapped a dog breeder to lead the pandemic response and suggesting people inject disinfectant – have become increasingly indiscernible from satire. It’s like ‘Tiger King’, but on healthcare.
In this tragic and farcical situation, the differences between the healthcare systems and approaches in the US and Cuba have become more apparent.
Cuba has long prioritized healthcare as a right that all people should have, while America believes that the market should dictate who has access and who doesn’t. Cuba has exported its doctors across the globe to help stem the pandemic’s tide, while the US has tightened the stranglehold on the island in a futile attempt to stop it from doing so.
The schism between the two is less a matter of money than a matter of philosophy. Cuba, for all its shortcomings, has maintained an indomitable commitment to the health and lives of people, and it has been vindicated during this pandemic.
Meanwhile, its wealthy neighbor to the north sinks deeper into a death spiral, intent on proving the superiority of the capitalist orthodoxy its government wants applied to every sphere of life, in every part of the planet.
Look, we won’t know the truth for many years but I for one will trust the Chinese more than the Americans. Americans lie too much and cannot be trusted.
Exclusive: US Army Brought COVID-19 to China with Fake ‘Military Games’ Team (March 12 story)
VT’s overall poor relationship with the Trump presidency has moved up a notch. The report Trump is referencing went, not unnoticed, but rather totally censored in the Western press, as has so much else until VT sought out the facts and published them.
Now, for the second time, Trump has made sad and silly denials, this one filled with hyperbole and grandiose behavior, typical of a spectrum sociopath.
March 12, 2020: In October 2019, the US brought 172 (really 369) military athletes to Wuhan for the World Military Games. Despite having the largest military in the world, tenfold, the US came in 35th behind nations like Iran, Finland and Slovenia. No video or photos exist of the US team, no records were kept, a huge team but a pitiful performance for the best military in the world.
The US team did so badly that they were called “Soy Sauce Soldiers” by the Chinese. In fact, many never participated in any event and stayed near the Huanan Seafood Wholesale Market, where the disease is said to have originated only days after the US left the area.
The US team went home on October 28, 2019, and within 2 weeks, the first human contact cases of COVID 19 were seen in Wuhan. The Chinese have not been able to find “patient zero” and believe he was a member of the US team.
They also have sources that say the US had misrepresented influenza that Trump claims have killed thousands, influenza carried to China by the US team, influenza that was really COVID 19, a disease developed in a military bio-warfare facility in the state of Washington, now “ground zero” in the US for COVID 19.
The Chinese claim, something censored in the US, that the inattentive attitude and disproportionately below average results of American athletes in the game indicates they might have been in for other purposes and they might actually be bio-warfare operatives, and that their place of residence during their stay in Wuhan was also close to the Huanan Seafood Wholesale Market, where the first known cluster of cases occurred.[28][29]
RT/Moscow: The US army might have brought the novel coronavirus disease (COVID-19) to China’s Wuhan, the city where the virus was first detected in the country, Chinese Foreign Ministry Spokesman Zhao Lijian said on Thursday.
“When did patient zero begin in the US? How many people are infected? What are the names of the hospitals? It might be the US army that brought the epidemic to Wuhan. Be transparent! Make public your data! The US owes us an explanation!” Zhao tweeted.
Chinese foreign ministry spokesperson Lijian Zhao has demanded US authorities reveal what they’re hiding about the origins of Covid-19, going as far as to suggest the coronavirus may have been brought to China by the US military.
Pointing to a video of the Centers for Disease Control and Prevention (CDC) director Robert Redfield apparently admitting the US had several deaths from Covid-19 before they were able to test for it, Zhao called on the American watchdog to come clean in a tweet posted on Thursday.
Lijian Zhao 赵立坚
✔@zlj517
2/2 CDC was caught on the spot. When did patient zero begin in US? How many people are infected? What are the names of the hospitals? It might be US army who brought the epidemic to Wuhan. Be transparent! Make public your data! US owe us an explanation!
“It might be US army who brought the epidemic to Wuhan,” Zhao suggested, calling for the CDC – and the US in general – to “be transparent” and share what they know about where and when “Patient Zero” was first diagnosed.
Aug 2019: US army biohazard labs shut down for failing safety checks.
The lab is in Washington State where they have highest incidence of COVID-19.
In the video, Redfield acknowledged that some cases of coronavirus were misclassified as influenza as the medics did not have an accurate test for the new epidemic at the time. He did not elaborate on when these misdiagnosed cases first appeared – saying only that “some cases have been diagnosed that way.”
Taro@taro_taylor
CDC director openly admitting that some #covid deaths have been misdiagnosed as influenza in the US. The question is when are those deaths. This supports the claims made by Japanese scientists that the virus originated from the US but was covered up.#COVID19#Corona
In the absence of any patients’ details or chronology of deaths, speculation has swirled. Zhao’s “theory” in particular focused on the military delegation that traveled to Wuhan in October for the Military World Games, weeks before the city confirmed the outbreak in December. The delegation was part of the 300-member group of American athletes taking part in the multi-sport event held every four years.
H.amirabdollahian@Amirabdolahian
The #Bahrain Interior Minister accused Iran of spreading #COVID19 & biological warfare. I respond to him that the #USA with its 5th fleet governing Bahrain is the main factor behind #BiologicalWarfare and even initial hiding #CoronavirusOutbreak in America.
Zhao is not the only high-profile political figure to voice suspicions about the timing of the Games and the introduction of the coronavirus in Wuhan. Former Malaysian PM Matthias Chang offered similar speculation back in January, zeroing in on the event as the launch point for what he deemed a biological war waged by the US against China.
Isaac Stone Fish
✔@isaacstonefish
·
Two things are true at the same time: Beijing deserves blame and censure for botching its handling of the coronavirus, which now endangers American lives. AND blaming or discriminating against Chinese people for the spread of the coronavirus is unethical, bad strategy, and nasty.
Chris Jiang@crs_1222
We are still figuring out where the virus originated. And chances are high that the virus was brought to China by the US army team who visited Wuhan in October. Anyway, no human deserves COVID-19. The world should fight against the disease together. No time for blame.
The World Health Organization (WHO) states that what is now the Covid-19 pandemic was first reported as a coronavirus outbreak in Wuhan, China, on 31 December 2019. The search for the deadly disease’s origin has been ongoing, with conflicting versions blaming the Wuhan food market and bats – a local delicacy – sold there in particular, while others opined humans might have gotten the virus from pangolins, an endangered scaly mammal.
Less orthodox theories suggest malicious intent, with the head of Iran’s elite Revolutionary Guards sensationally claiming last week that Covid-19 could possibly be “a product of a biological attack by America which initially spread to China and then to Iran and the rest of the world.”
So far, the problem with all of those theories, blaming both animals and humans, is that no direct causal proof has been established, while the identity of China’s “patient zero” also remains unclear. And it’s not China alone: in Washington state – which seemingly identified and successfully isolated its first infected traveler, with dozens of contacts identified and monitored – the virus somehow began spreading anyway. Even Steve Wozniak, Apple’s co-founder, at one point claimed he and his wife may have been the US’ “patient zero” after developing a bad cough on return from China. It has since emerged his wife’s diagnosis was “a sinus infection,” however.
From October 18 to October 27, 2019, the World Military Games was held in Wuhan, and the United States sent 369 soy sauce soldiers to participate.
Why is it soy sauce soldiers?
Because in the 10-day game, the performance of the American soy sauce soldiers was so disappointing that even Bahrain was unnecessarily disappointed, the gold medal was even missing, and the overall score was left far behind by North Korea, which once gave Mexico a chance. The urge to counterattack the continental United States.
However, the poor performance in the game did not affect the mood of the soy sauce soldiers playing in Wuhan.
They teamed up in groups of two, and played around the streets of Wuhan, leaving many romantic accidents.
It should be pointed out that the location of the US guest house of the Military Games is not far from South China Seafood City.
At the end of the military games, just when people were wondering, how could these gangsters who ca n’t wait to build muscles on their faces suddenly get fired up? Did the American soldiers ’food only be grappled? Or did they forget to eat it during the game? Snickers?
Gordon Duff is a Marine combat veteran of the Vietnam War. He is a disabled veteran and has worked on veterans and POW issues for decades. Gordon is an accredited diplomat and is generally accepted as one of the top global intelligence specialists. He manages the world’s largest private intelligence organization and regularly consults with governments challenged by security issues.
Duff has traveled extensively, is published around the world and is a regular guest on TV and radio in more than “several” countries. He is also a trained chef, wine enthusiast, avid motorcyclist and gunsmith specializing in historical weapons and restoration. Business experience and interests are in energy and defense technology.
A Swiss medical doctor provided the following information on the current situation in order to enable our readers to make a realistic risk assessment. (Below you will find regular, but not daily, updates on medical and political developments.)
***
According to the latest data of the Italian National Health Institute ISS, the average age of the positively-tested deceased in Italy is currently about 81 years. 10% of the deceased are over 90 years old. 90% of the deceased are over 70 years old.
80% of the deceased had suffered from two or more chronic diseases. 50% of the deceased had suffered from three or more chronic diseases. The chronic diseases include in particular cardiovascular problems, diabetes, respiratory problems and cancer.
Less than 1% of the deceased were healthy persons, i.e. persons without pre-existing chronic diseases. Only about 30% of the deceased are women.
The Italian Institute of Health moreover distinguishes between those who died from the coronavirus and those who died with the coronavirus. In many cases it is not yet clear whether the persons died from the virus or from their pre-existing chronic diseases or from a combination of both.
The two Italians deceased under 40 years of age (both 39 years old) were a cancer patient and a diabetes patient with additional complications. In these cases, too, the exact cause of death was not yet clear (i.e. if from the virus or from their pre-existing diseases).
The partial overloading of the hospitals is due to the general rush of patients and the increased number of patients requiring special or intensive care. In particular, the aim is to stabilize respiratory function and, in severe cases, to provide anti-viral therapies.
(Update: The Italian National Institute of Health published a statistical report on test-positive patients and deceased, confirming the above data.)
The doctor also points out the following aspects:
Northern Italy has one of the oldest populations and the worst air quality in Europe, which has already led to an increased number of respiratory diseases and deaths in the past and is likely an additional risk factor in the current epidemic.
South Korea, for instance, has experienced a much milder course than Italy and has already passed the peak of the epidemic. In South Korea, only about 70 deaths with a positive test result have been reported so far. As in Italy, those affected were mostly high-risk patients.
The few dozen test-positive Swiss deaths so far were also high-risk patients with chronic diseases, an average age of more than 80 years and a maximum age of 97 years, whose exact cause of death, i.e. from the virus or from their pre-existing diseases, is not yet known.
Furthermore, according to a first Chinese study, the internationally used virus test kits may give a false positive result in some cases. In these cases, the persons may not have contracted the new coronavirus, but presumably one of the many existing human coronaviruses that are part of the annual (and currently ongoing) common cold and flu epidemics. (1)
Thus the most important indicator for judging the danger of the disease is not the frequently reported number of positively-tested persons and deaths, but the number of persons actually and unexpectedly developing or dying from pneumonia (so-called excess mortality).
According to all current data, for the healthy general population of school and working age, a mild to moderate course of the Covid-19 disease can be expected. Senior citizens and persons with existing chronic diseases should be protected. The medical capacities should be optimally prepared.
Important reference values include the number of annual flu deaths, which is up to 8,000 in Italy and up to 60,000 in the US; normal overall mortality, which in Italy is up to 2,000 deaths per day; and the average number of pneumonia cases per year, which in Italy is over 120,000.
Current all-cause mortality in Europe and in Italy is still normal or even below-average. Any excess mortality due to Covid-19 should become visible in the European monitoring charts.
Winter smog (NO2) in Northern Italy in February 2020 (ESA)


















{kind=link}